
Written and reviewed by
Antonia Moosmann
Psychologist in Germany, M.Sc. Clinical Psychology. I write these guides the way I'd answer the question if you asked me in person — naming what the evidence supports, what it doesn't, and where the marketing runs ahead of the research.
Read more about how I reviewKey facts
In a hurry? Here's the short version.
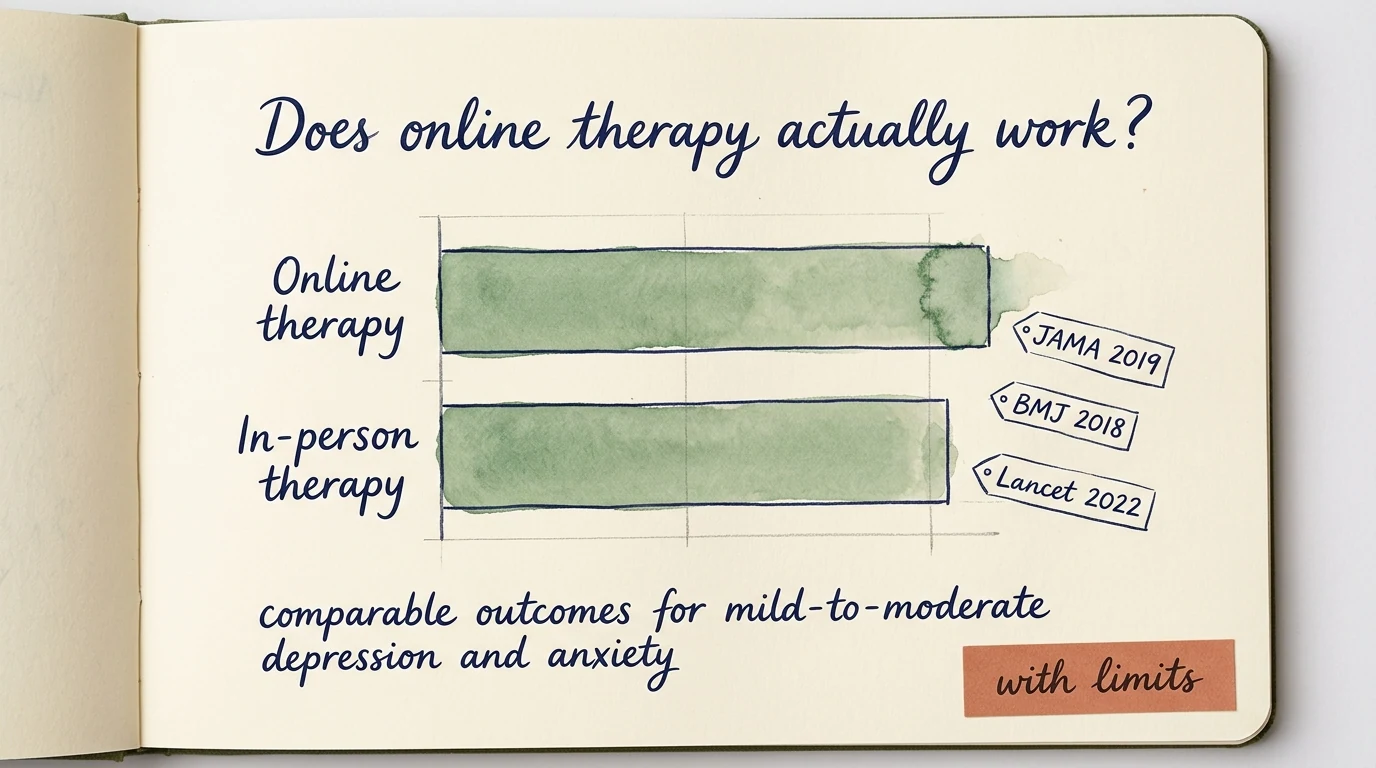
- Yes, in the trial conditions where it's been studied most. Structured online cognitive behavioural therapy — iCBT — shows roughly comparable outcomes to face-to-face CBT for adult depression, anxiety, and panic disorder across many meta-analyses.
- But what's been studied isn't always what's being sold. Most of the published evidence is on manualised iCBT programs in research and public-health settings, not on subscription messaging platforms (BetterHelp, Talkspace, Online-Therapy.com) that dominate the consumer market.
- Online is a strong fit when access or scheduling is the bottleneck, when symptoms are mild-to-moderate, or when you write well and like working asynchronously.
- It's a poor fit for active crisis, complex trauma, severe symptoms, or anything needing close real-time monitoring. If you're in danger, please use a crisis line first: 988 (US), Samaritans (UK), or Telefonseelsorge 0800 111 0 111 (Germany).
- Where to go next: for a platform-level look, see the BetterHelp review — strengths, limits, and when I'd point readers elsewhere.
"Online therapy works" is a true sentence about a body of research. "BetterHelp works" is a different sentence with much less evidence behind it. I keep getting asked the first one when people really want the answer to the second.
Start here
What people actually mean by "online therapy"
The honest first move is to notice that "online therapy" isn't one product — it's four. They have different evidence profiles and different price tags. When someone asks me whether online therapy works, the useful answer starts by asking which of these they're actually asking about.
| Format | What you actually get | Evidence base | Best for |
|---|---|---|---|
| Live video therapy | Scheduled 50-minute video call with a licensed clinician. | Strong. | Most general-practice problems; closest analogue to in-person. |
| Structured iCBT | 6–12 modules, clinician-guided, weekly check-ins, homework. | Strongest of any online format. | Depression, anxiety, panic, social anxiety, OCD. |
| Messaging-first platforms | Text-thread relationship + optional live sessions on top. | Thinner — mostly company-funded outcome data. | Mild-to-moderate symptoms, scheduling-blocked clients, writers. |
| App-based coaching | Self-guided exercises with optional human coach. | Adjacent to therapy, not a substitute. | Self-help adjunct, stress, sleep, daily check-ins. |
When the meta-analyses say "online therapy works," they are mostly speaking about live video and structured iCBT. That distinction matters for the rest of this page.
The evidence
What the research actually shows
Most of the encouraging headlines trace back to one body of evidence: internet-delivered cognitive behavioural therapy, usually written as iCBT. Across more than a decade of meta-analyses — the long tradition led by Gerhard Andersson, Per Carlbring, Erik Hedman and colleagues — structured iCBT shows outcomes broadly comparable to face-to-face CBT for adult depression, generalised anxiety, panic disorder, social anxiety, and OCD.
The American Psychological Association's position on telepsychology is, simplified: when ethical and clinical standards are met, video-delivered therapy is empirically supported as a delivery format — not a watered-down version of the real thing.
The Cochrane reviews that exist say roughly the same thing with more hedging: moderate-quality evidence for benefit, with the usual caveats about study heterogeneity.
That's a real finding. It's also a finding with a lot of fine print — which is where the next section comes in.
The caveat
Where the research is thinner than it looks
Here is the part that almost never makes it into a marketing page: what's been studied is not always what you're buying.
The well-evidenced format is structured, manualised iCBT — programs with defined modules, a clinician guiding the work, weekly check-ins, and homework. Often run inside a research trial, sometimes inside a public-health system (the UK's Talking Therapies, parts of the Swedish system, a few Australian programs).
A subscription messaging platform is a different product altogether. Here's the gap laid out:
| Dimension | Research-grade iCBT | Commercial messaging platforms |
|---|---|---|
| Who delivers it | Trained clinicians, often inside a research trial or public-health program. | Licensed clinicians on a marketplace, with much less protocol oversight. |
| Structure | Manualised — defined modules, sequence, dosage. | Whatever you and your therapist agree to. Often unstructured messaging. |
| Relationship format | Weekly video or asynchronous check-ins inside a defined program. | Mostly text. Live sessions cost extra on most plans. |
| Evidence base | Dozens of independent meta-analyses since ~2014. | Mostly company-funded studies; independent evaluation is thin. |
| Who it's been studied on | Mild-to-moderate, motivated, often English-speaking, often selected. | Wider, self-selected; less rigorous outcome tracking. |
That doesn't mean platforms don't help anyone. Plenty of people get real benefit from them. It means the move from "online therapy works" to "BetterHelp works" is a longer leap than the marketing implies.
When I'm asked, I name that gap rather than smooth it over.
Match the format to your actual life, not your aspirations. The best therapy is the one you'll show up for.
When it fits
When online therapy is a good fit
I'd default to online when one or more of the following is true, and you've already ruled out crisis-level symptoms (see the safety section below).
- Geography is the bottleneck
Rural areas, smaller cities, or any place where in-person availability is essentially zero. Online dramatically widens the clinician pool you can actually reach.
- Scheduling is the bottleneck
Shift work, caregiving, travel, neurodivergent energy budgets. A 7 a.m. or 9 p.m. slot from home beats the in-person session you keep cancelling.
- Mild-to-moderate, focused symptoms
Anxiety, low mood, sleep difficulty, a specific phobia, work stress, mild OCD. The research is strongest on these profiles.
- You write well and like writing
Async messaging favours people who think on the page. If composing a paragraph is easier than improvising aloud, the format works with you.
- Step-up or step-down
A useful step-up from a workbook or self-help app, and a reasonable step-down from intensive in-person work.
When it doesn't
When online therapy is a poor fit
These are the situations where I'd push back if a client suggested starting online — not because online care is bad, but because the format doesn't fit the problem.
- Active suicidal ideation, self-harm, or recent attempt
Crisis care needs a clinician who can act in real time, not a 24-hour reply window. Use crisis lines and seek in-person or specialist care.
- Complex trauma
The therapeutic relationship, body awareness, and a steady physical container matter. A screen is a real limitation here.
- Severe symptoms or instability
Acute psychosis, severe eating disorders, active substance use disorders requiring monitoring — these need more oversight than typical platforms offer.
- Medication needs you can't fill remotely
Controlled substances especially. Rules vary by country and US state. Check before assuming a platform's prescribers can cover what you need.
- You'd dread opening the app
If you'd quietly cancel every session, you'll decide therapy doesn't work. Match the format to your actual preferences, not your aspirations.
Decision making
How I'd actually think about choosing
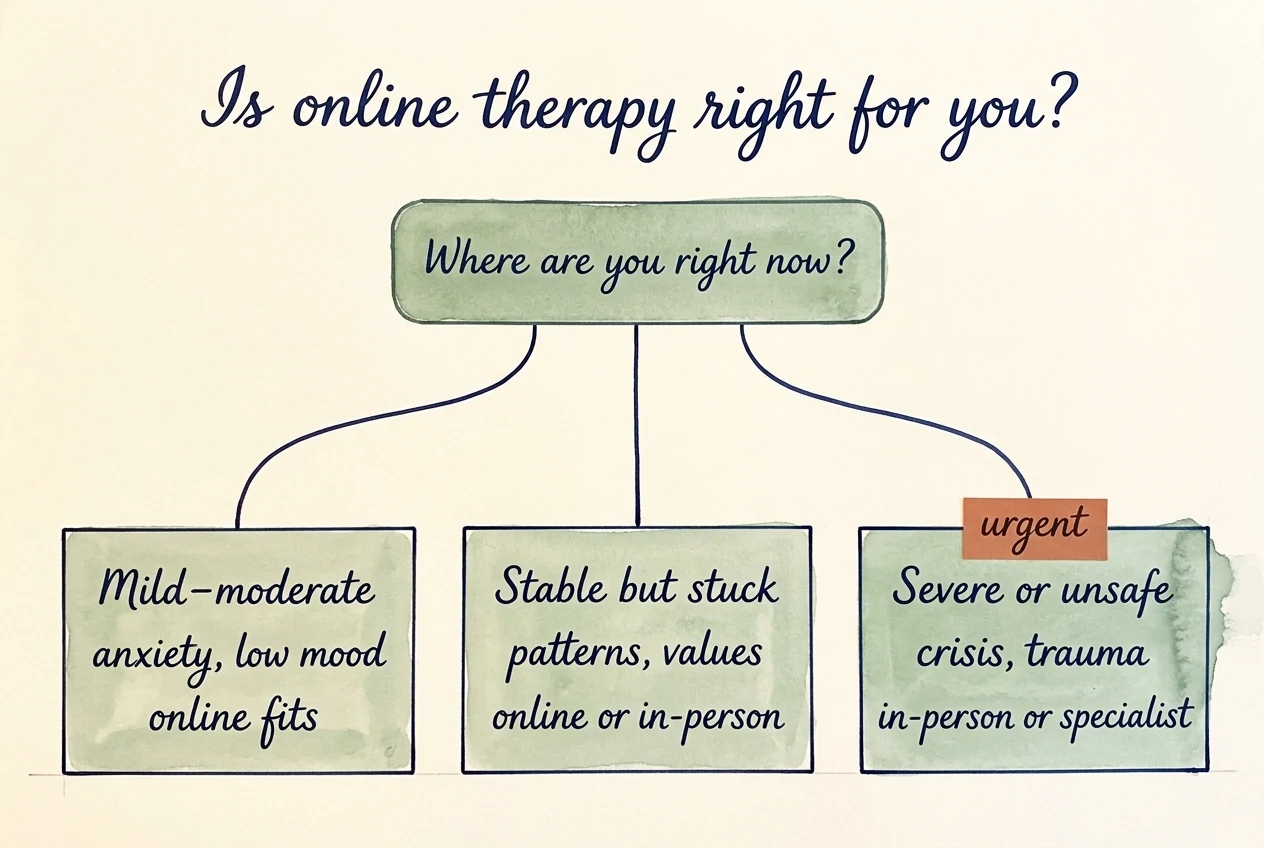
Three filters, in this order, are how I'd run the decision myself.
Filter 1
What kind of problem are you bringing?
If it's specific and skills-based — anxiety, sleep, low mood, a phobia — a structured CBT-flavoured platform or live-video therapy is the strongest fit. If it's relational, exploratory, or trauma-related, weight live video over messaging, and weight in-person over both if you can swing it.
Filter 2
What kind of access do you have?
If in-person isn't available within an hour of you, or your schedule doesn't survive a fixed weekly daytime slot, online stops being a compromise and starts being the actual best fit.
Filter 3
What kind of evidence do you trust?
If you want the strongest published outcomes, pick a structured iCBT program or a live-video service with credentialed clinicians. If you're choosing a messaging-first commercial platform, do it with eyes open: the platform's published outcomes are usually their own, the format suits some problems better than others, and you can leave if it isn't working.
A note on sources
The summary above leans on the long meta-analytic tradition on internet-delivered CBT (Andersson, Carlbring, Hedman and colleagues, with steady output from roughly 2014 onward), the American Psychological Association's guidance on telepsychology and digital mental health , and the Cochrane reviews on remotely delivered psychological therapy.
I've tried to summarise where the evidence is strong and where it isn't, rather than cite single studies as if they settle a question — the honest picture is many studies, broadly pointing the same direction, with the caveats I named above.
For platform-specific evidence and what to actually do with it, see the online therapy comparison and the individual platform reviews from there.
Common questions
Is online therapy as effective as in-person therapy?
For mild-to-moderate depression and anxiety, structured iCBT and live-video therapy have shown roughly comparable outcomes to in-person CBT across many meta-analyses. For complex, relational, or trauma-focused work, the evidence base is thinner and in-person tends to retain advantages. Saying "as effective" without specifying the population, the format, and the problem is overclaiming.
Are BetterHelp and Talkspace research-backed?
The broader category of online therapy is research-backed. The specific commercial messaging platforms have published far less peer-reviewed independent outcome data than that broader literature implies. Most published evaluations of BetterHelp or Talkspace are company-funded. That doesn't make them bad — but "online therapy works" is a stronger claim than "BetterHelp works," and you should weight the difference when reading their marketing.
Does insurance cover online therapy?
In the US, many insurance plans now cover telehealth therapy at parity with in-person, but the major subscription platforms (BetterHelp, Talkspace, Online-Therapy.com) are often out-of-network or self-pay. Talkspace has more in-network coverage than the others. Outside the US, public-health systems (NHS Talking Therapies in the UK, parts of the German and Swedish systems) include iCBT options at no direct cost — usually with a referral or self-referral pathway.
Can an online therapist prescribe medication?
Sometimes. Platforms with psychiatry tracks (Talkspace Psychiatry, Brightside, Cerebral and similar) can prescribe many medications remotely. Controlled substances have stricter rules that vary by country and by US state, and the regulatory landscape has been moving. If medication management is the main thing you need, confirm what the platform can actually prescribe in your jurisdiction before signing up.
I'm in Germany — does any of this apply?
Partially. German online-therapy regulation (especially video sessions reimbursed by gesetzliche Krankenkassen) is its own world, and many US-focused platforms either don't operate or operate as self-pay. The iCBT effectiveness research applies internationally; the platform-specific guidance on this page is mostly US-focused. A German-language version of this page is on the way.
What if I try it and it isn't helping?
Give a new therapist three to five sessions to settle, not one. After that, if the fit is wrong, name it directly — most therapists would rather you switched than quietly disengaged. "This format isn't working for me" or "I'd like to try someone with a different style" is a complete sentence. Online platforms generally make switching easier than in-person referrals; that's one real advantage they have.